A new act in Canada bans non-citizens, non-permanent residents and foreign commercial enterprises from buying Canadian residential properties. (Shutterstock) Diana…
Agency ReportKindly share this story:A six-year-old boy opened fire in an elementary school classroom in the eastern US state of Virginia on Friday, seriously injuring a teacher, police said.No students were hurt in the incident at Richneck Elementary School in the coastal city of Newport News.
“The individual is a six-year-old student. He is right now in police custody,” local police chief Steve Drew told a news conference, adding that “this was not an accidental shooting.”Police said that the victim was a teacher in her 30s and her injuries were believed to be life-threatening.Imagine such, how did he get the gun & having the mind to shoot at someone. The influence Wahala wahala wahala Wahala..and the boy will go scot free las las Shits
After four days of lobbying and facing opposition from members of his party, Mr McCarthy clinched the highly envied seat with 216 votes.
The US parliament on Saturday elected Republican Kevin McCarthy as Speaker after 15 historic ballots.
After four days of lobbying and facing opposition from members of his party (Republican Party), who the US media nicknamed the ‘Never Kevins’, Mr McCarthy clinched the highly envied seat with 216 votes; putting him ahead of his competitor, Hakeem Jeffries, a democrat who got 212 votes.
The new Speaker’s emergence came at a price including allowing any member of parliament to move for his removal from office.
Other compromises made by Mr McCarthy, according to CNN, include moving 12 appropriations bills individually. Instead of passing separate bills to fund government operations, Congress frequently passes a massive year-end spending package known as an “omnibus” that rolls everything into one bill.
Conservatives rail against this, arguing that it evades oversight and allows lawmakers to stick in extraneous pet projects.
He also agreed to more Freedom Caucus representation on committees, including the powerful House Rules Committee. Also, lawmakers will have seventy-two hours to review bills before they come to floor.
An investigative committee will be created to probe the “weaponisation” of the federal government; and restoring the Holman rule, which can be used to reduce the salary of government officials.
While many argue that Mr McCarthy’s compromises could end up making him a weak leader in one of the strongest political seats, AP argues that he could also be emboldened as a survivor of one of the more brutal fights for the gavel in US history.
“Not since the Civil War era has a speaker’s vote dragged through so many rounds of voting,” AP said.
McCarthy as speaker
In a tweet after his emergence, he tweeted “I hope one thing is clear after this week: I will never give up. And I will never give up for you, the American people.”
In his speech Saturday morning after he emerged, the hard work begins, he said, adding that his ultimate responsibility is not to his party, or the congress but to the US – “our country.”
The new Speaker said it was time for the parliament to be a check and provide balance to President Joe Biden’s policies.
As part of his plans for his tenure, Mr McCarthy intends to win the economic competition with China by bringing back jobs that were taken by the latter.
“As for the Chinese Communist Party, we will create a bipartisan select committee on China to investigate how to bring back the hundreds of thousands of jobs that went to China and then we will win this economic competition,” he said.
A new law will erode public oversight into police misconduct. In this July 2021 photo, police are seen clearing a homeless encampment in Toronto. THE CANADIAN PRESS/Chris Young
Changes to how public complaints against police officers are handled will make the complaints system even more insular in Ontario.
Through the province’s Community Safety and Policing Act, 2019, the system for handling non-criminal police misconduct will quietly shift a greater portion of the system out of the public eye.
It broke ground as the first and only independent systemic review of the police oversight system to tackle how complaints against police officers and police officer discipline are handled.
Although some recommendations were adopted through the 2019 act, most were not.
Independent investigations
The OIPRD has been in charge of handling public complaints against the police since it was established in 2007. It is Ontario’s independent police watchdog on matters of non-criminal police misconduct. The Special Investigations Unit, on the other hand, conducts investigations of incidents involving the police that have resulted in death, serious injury or allegations of sexual assault.
In this role, the OIPRD co-ordinates with police forces in Ontario to manage the complaints intake and screening process. It also publishes the results of police misconduct hearings on its website.
The OIPRD can conduct misconduct investigations by itself. However, the police forces themselves take on the majority of duties associated with those investigations.
A key recommendation was that complaints investigations should no longer be handled by police forces.
A new name in police complaints probes
Currently, individual police services conduct most investigations into complaints about police officers, and this will increase as a result of the 2019 act.
The OIPRD summarized the forthcoming changes on its website, explaining how it will be renamed the Law Enforcement Complaints Agency.
The agency’s Complaints Director will conduct investigations into public complaints about police chiefs and deputy chiefs, other high-ranking officers and “any other complaints determined to be in the public interest.”
But “all other complaints will be referred back to either the police service from which they originated or another police service.”
Such a change shrinks the role of independent oversight into police misconduct.
Transparency and public trust in the system
Tulloch’s report cautioned that the current system sets up public complainants for disappointment.
At the conclusion of an investigation, the investigator makes a crucial decision about whether the misconduct allegations associated with a complaint are substantiated. This decision cannot be appealed.
A CBC investigation found that out of all the complaints made against Toronto police officers from 2014 to 2019, only two per cent were substantiated. Only one per cent of substantiated complaints have gone before the Toronto police disciplinary tribunal.
Even for substantiated complaints that go before a disciplinary tribunal, disciplinary action against the police officer is not guaranteed.
As a result of the 2019 act, a more limited range of police disciplinary matters will be settled through a hearing, the only public venue for adjudicating police misconduct. These changes erode public trust in the system.
Many complainants find that the system lacks transparency, especially at the police discipline stage. Members of the public have limited avenues for learning about how police forces address individual issues of police misconduct, let alone service-wide trends.
Human rights monitoring in Ontario
One of the most troubling consequences of the current system is that it prevents public agencies from monitoring systemic racism and other human rights abuses associated with non-criminal police misconduct.
According to the commission, confidentiality provisions in Ontario’s policing laws “prevent the public from knowing when and whether an officer was subject to some form of discipline for engaging in racial profiling, racial discrimination or other police misconduct.”
People protest to defund the police in front of Toronto Police Service headquarters in July 2020.THE CANADIAN PRESS/Nathan Denette
The changes from the new Ontario law will make it even harder to monitor police officer violations of human rights. These changes undermine the essential public purpose of the system.
Defence Minister Anita Anand holds a media availability on Parliament Hill in December 2022 on her report to Parliament on culture change reforms at the Canadian Armed Forces. It’s the latest of many pledges to reform the CAF’s culture. THE CANADIAN PRESS/Sean Kilpatrick
Sexual violence in the Canadian Armed Forces (CAF) is a common, dominant and serious issue that has severe consequences for victims — not to mention its impact on unit cohesion and morale.
Workplace violence is an ever present issue in Canadian society, impacting nearly three-quarters of Canada’s workers. Measures must be taken to treat any workplace violence as a public health issue.
But the impenetrable closed culture of the CAF in particular is prime real estate for predators and those who seek to abuse authority.
Canada set aside close to $800 million in 2019 to settle class-action lawsuits by current and former military members involving sexual misconduct. What’s lacking, however, is a coherent national strategy to prevent, address and reset the culture of sexualized violence within the CAF.
Anand’s first move
In November 2021, Defence Minister Anita Anand’s first act was to announce the transfer of the investigation and prosecution of sexual misconduct cases from within the Canadian Forces to the civilian justice system.
One year later, on Dec. 13, 2022, Anand stepped in front of the cameras to apologize to former and current members of the CAF for the culture of violence and to those who have survived sexual misconduct and assault. The apology was likely meant as a meaningful step towards reconciliation.
Her comment, however, that “this time is different,” raises concerns. The question becomes: “How so, and why should we believe the government this time?”
Marie Deschamps, former Supreme Court justice, attends a committee on the external review into sexual misconduct and sexual harassment in the Canadian Armed Forces in May 2015.THE CANADIAN PRESS/Sean Kilpatrick
Organizational culture is often so firmly entrenched that changes in strategy have little impact. So Anand is sounding like a broken record because the CAF’s traditions, culture and much of its toxic leadership haven’t changed.
In 2015 — almost a decade ago — the CAF released an external report detailing the results of a survey on sexual misconduct in the organization conducted by Marie Deschamps, a former Supreme Court justice.
The survey found that women in the CAF endure a toxic work environment and are often the target of vulgar name-calling, sexual innuendo and jokes, harassment and assault — much of it condoned or ignored by senior military leaders. The track record of the CAF’s leadership in dealing with the issue of sexual misconduct, as well as ministerial oversight, is abysmal.
The CAF’s response
In response to the 2015 survey, the CAF implemented several initiatives aimed at addressing sexual misconduct in the organization, including creating a Sexual Misconduct Response Centre (SMRC) and appointing a Special Advisor on Sexual Misconduct.
The Special Advisor works with the CAF to identify and address the root causes of sexual misconduct and to develop and implement strategies to prevent it. Clearly this arrangement hasn’t been working.
The CAF also implemented a policy called Operation HONOUR, referred to as an enduring mission with no end date by Lt.-Gen. Mike Rouleau, with a plan to eliminate sexual misconduct in the military and support survivors. At this point, that mission has also been a failure.
Former top commander Jonathan Vance pleaded guilty in 2022 to criminal charges related to accusations that he committed sexual misconduct when leading the Armed Forces, despite stating that sexual misconduct was “a threat to this institution.”
Jonathan Vance sits in the front row during a news conference in June 2020 before he left the military in March 2022.THE CANADIAN PRESS/Adrian Wyld
In 2018, the CAF released a report on the progress made in addressing sexual misconduct in the organization.
It found that the number of reported sexual assaults had increased, in some ways a positive development because it indicated more survivors were coming forward and seeking support. The findings suggest the CAF has made some progress in increasing awareness of sexual misconduct and improving support for victims, but the organization’s culture is clearly not changing at all.
The enemy is in the same uniform
So now what?
As someone who specializes in workplace violence, it occurred to me that if I were a parent of a child who was contemplating a career in the CAF, I would need to have a difficult conversation about the likelihood of sexual assault.
Sit with that for a minute. When we think about the CAF, we acknowledge the duty, honour and courage of most of those who serve. However, the clear and present danger is not just in distant battlefields — but also from those serving in the same uniform as you.
The likelihood of adverse mental health outcomes — including anxiety, depression and PTSD — may not just come from what is experienced in battle but what is inflicted by a brother or sister in arms, severely impacting the trust, credibility and honour of the CAF.
The CAF has created a restricted culture with a leadership team lacking in diversity, inclusion and the considerations of equity. These leaders have learned from others who have perpetrated sexual misconduct.
Prevention, intervention and post-intervention measures for dealing with sexualized violence in the CAF are not considered mission-critical by the organization — but they need to be.
So is this time different? Is genuine culture change truly on the near horizon at the CAF? I hope so, but unfortunately hope is not a strategy.
Federal Health Minister Jean-Yves Duclos, Mental Health and Addictions Minister and Associate Minister of Health Carolyn Bennett and MP Nathaniel Erskine-Smith (right) listen as Morris Rosenberg, chair of the independent review board on the impact of legalization of cannabis, speaks at a news conference in Ottawa on Sept. 22. THE CANADIAN PRESS/Adrian Wyld
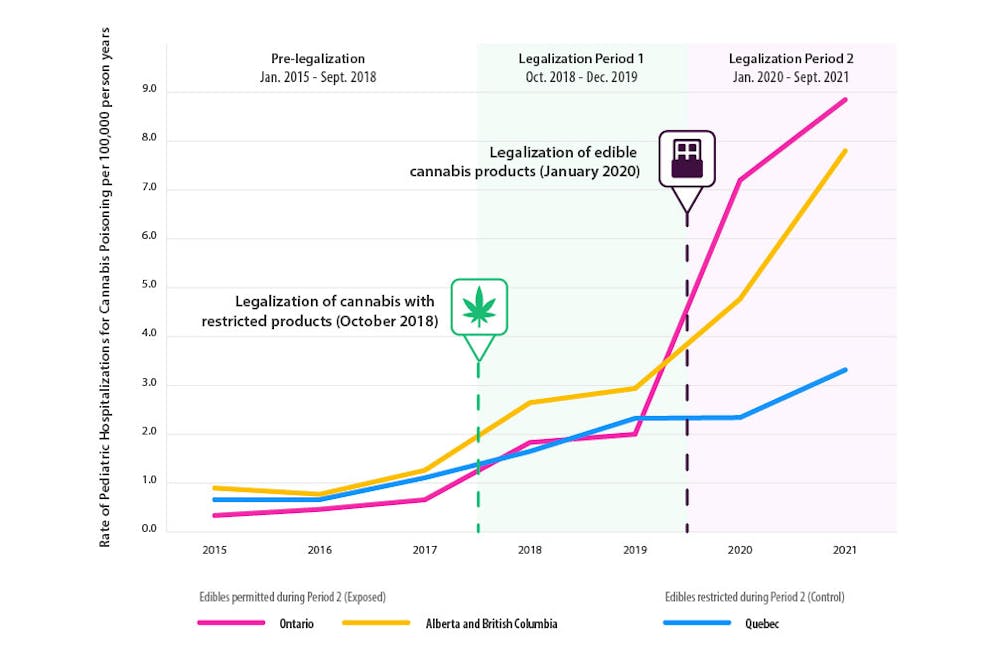
When Canada legalized non-medical cannabisfour years ago, there was enormous uncertainty about how legalization could impact the health of Canadians. Since then, there has been increasing evidence that legalization has resulted in some negative health effects. The clearest of these is a large increase in accidental cannabis poisonings in young children.
We conducted two large studies that found a nine-fold increase in emergency department visits and a six-fold increase in hospitalizations for cannabis poisoning in children younger than 10 years (average age of 3.5 years) following cannabis legalization in Canada. These increases have been so substantial that cannabis is now a leading cause of hospitalizations for poisoning in this age group.
Looking at the provincial variation in the ways that legalization was implemented across Canada, it’s clear that increases in cannabis poisonings in young children did not need to occur.
At the start of legalization in October 2018, the federal government only allowed the sale of dried cannabis flower. After an intentional one-year delay, new products, including cannabis edibles like candies and chocolates, were permitted.
Most of the increase in cannabis poisonings in young kids happened after edible products came to market. The increase was much more modest in Québec, where the sale of these products was prohibited.(Daniel Myran, Yaron Finkelstein), Author provided
A wide variety of these edibles went on sale everywhere in Canada except in Québec, which prohibited anything in the form of chocolates, gummies and candies based on concern over their high appeal to children.
We found that most of the increase in cannabis poisonings in young kids happened after edible products came to market, and that Québec — which prohibited their sale — was protected from this effect and saw a much more modest increase in pediatric cannabis poisonings.
This lack of increase in Québec strongly argues against alternative explanations, including that these hospital visits are from illegal cannabis products, caregivers becoming more comfortable disclosing that kids may have ingested cannabis or pandemic influences.
Child cannabis poisonings
When we care for infants and young children who have been rushed to the hospital for cannabis poisoning, we see many parents and caregivers who are shocked by the severity of the cannabis effects on their intoxicated child. Children can become very sick, be less responsive and in severe cases suffer from seizures, trouble breathing on their own, or even enter a coma.
With no effective antidote, children with severe cannabis poisoning require hospitalization — sometimes in intensive care units requiring a breathing machine — until the cannabis is processed and cleared from their body. The long-term effects of these unintentional poisonings are unknown.
It’s important to note the cannabis industry is specifically asking that many of these regulations — including THC limits and child-resistant packaging — be removed to make their products more competitive with the illicit market.
A variety of cannabis edibles are displayed at the Ontario Cannabis Store in Toronto on Jan. 3, 2020.THE CANADIAN PRESS/Tijana Martin
But legalization is not shaping up to be just about replacing the illegal market. The legal market is expanding far faster than the illegal market contracts. Canadian households now spend an estimated 37.3 per cent more on cannabis from all sources (medical, legal non-medical and illegal) than they did before legalization (1.44 billion in the third quarter of 2018 vs 1.93 billion in the second quarter of 2022). That means that we, as a country, are likely using increasing quantities of cannabis.
Youth cannabis use and harms
A key goal of legalization was to reduce cannabis use and related harms in youth. While the data is less definitive, there is also some reason for concern that these harms have increased.
The largest increases in emergency department visits due to cannabis occurred when the legal market began carrying new high-potency products and the number of cannabis retail stores rapidly expanded. These increases overlapped with much of the COVID-19 pandemic so it is hard to disentangle whether they reflect changes from legalization, a response to COVID-19 related stressors or a combination.
Social benefits of legalization
Increases in cannabis harms in young children and youth do not negate the social benefits of cannabis policy reform. Criminalization of cannabis created major problems, including life-altering limits on employment, education and financial opportunities. These effects were well documented to be heavily discriminatory due to over-policing among racialized communities and Indigenous youth.
Reducing criminal justice harms is of considerable public health interest. However, we argue that it does not necessitate cannabis commercialization that includes cannabis marketing, widespread cannabis retail stores and permitting ultra-high-potency products that appeal to youth and children.
As the federal government reviews the impacts of legalization to date, we recommend protecting the health of Canadian children and youth by — at a minimum — maintaining existing regulations. This includes plain and child-resistant packaging and THC content limits on edibles. Without these, we will almost certainly see greater numbers and far more severe cannabis poisonings in children.
While we examine more evidence on the impacts of legalization on younger Canadians, we also caution against loosening current rules that limit cannabis marketing and advertising which can appeal to youth and young adults.
If we want to reduce cannabis poisonings in children, we should consider further national restrictions on the taste and visual appearance of edibles and the type of edibles approved, as Québec has implemented.
Dec. 1 marks World AIDS Day. As researchers focused on fighting the HIV-AIDS epidemic, we are increasingly concerned all the progress made in the fight against the virus is at risk.
In 1996, the first remarkable breakthrough against the HIV-AIDS epidemic came with the novel combination of drugs that became known as Highly Active Antiretroviral Therapy (HAART).
For the first time, HAART was able to stop viral replication and render the virus undetectable in blood and bodily fluids, and consequently promote immune reconstitution. This in turn would prevent an HIV infection from developing into AIDS, significantly reducing premature deaths.
Treatment as prevention
The next major breakthrough came in the early 2000s. Through close monitoring of the epidemic in British Columbia, our research documented that HIV infected individuals who have consistent viral suppression with HAART are virtually unable to transmit the infection. This led us to recommend initiating HAART immediately following HIV diagnosis to accelerate overall HIV/AIDS control.
We called the strategy Treatment as Prevention (TasP) to illustrate the fact that HAART simultaneously stops progression to AIDS, premature death and HIV transmission.
TasP was enthusiastically embraced by the Joint United Nations (UN) Programme on HIV/AIDS (UNAIDS), in 2010. However, it soon became apparent that the TasP strategy was too ill defined, and this open the door for it to be inconsistently deployed between regions.
In 2014, UNAIDS unveiled two sequential TasP-inspired targets to quantify the proportion of people living with HIV who need to be diagnosed, the proportion of diagnosed people who need to be on HAART, and the proportion of people on HAART who need to be virologically suppressed by 2020 and 2025. Viral suppression is defined by having less than 200 copies of HIV per milliliter of blood.
Canada has made breakthroughs in the fight against HIV-AIDS, but more must be done to make access to treatment more equitable.THE CANADIAN PRESS/Justin Tang
These targets were specifically designed so that by 2030 the world would see a 90 per cent decrease in AIDS mortality and new HIV infections, and meet the goal of ending the HIV-AIDS pandemic. In 2015, the UN formally endorsed the 90-90-90 by 2020 target. It endorsed our subsequent 95-95-95 by 2025 target in 2021.
However, a lack of leadership and resources have hampered progress towards the UN targets around the world. This has been exacerbated by the COVID-19 pandemic, which disrupted some medical services, decreased HIV testing, interrupted the provision of HAART and diverted funding.
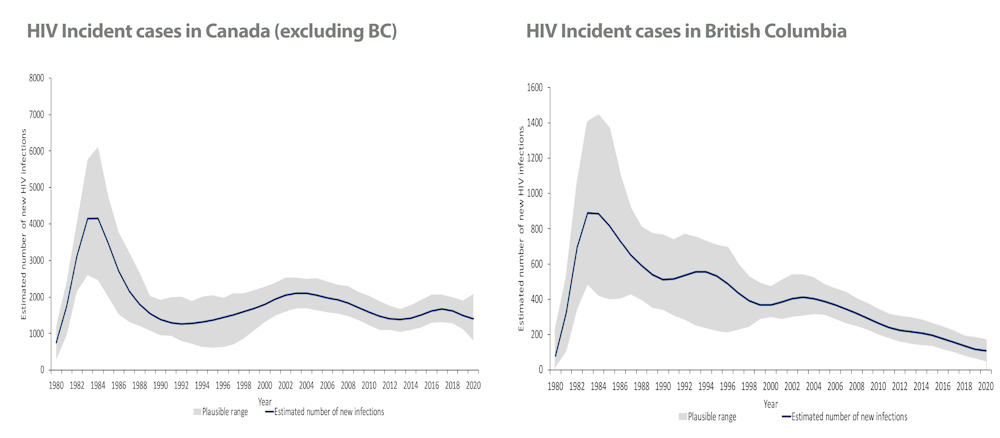
Unfortunately, the results were rather concerning. HIV cases in Canada have remained flat since the 1990s, but there is a marked contrast between British Columbia and the rest of the country. While B.C. saw a steady decline in cases between 1996 and 2020, the rest of Canada saw no further reduction in cases over the same period.
HIV cases peaked throughout Canada in the early 80s. But a decrease in high-risk sexual practices led to a substantial reduction in cases. After that, the course of the epidemics diverged.
HIV cases from 1980 until 2020 in Canada and British Columbia.(Public Health Agency of Canada 2020 National HIV Estimates Report)
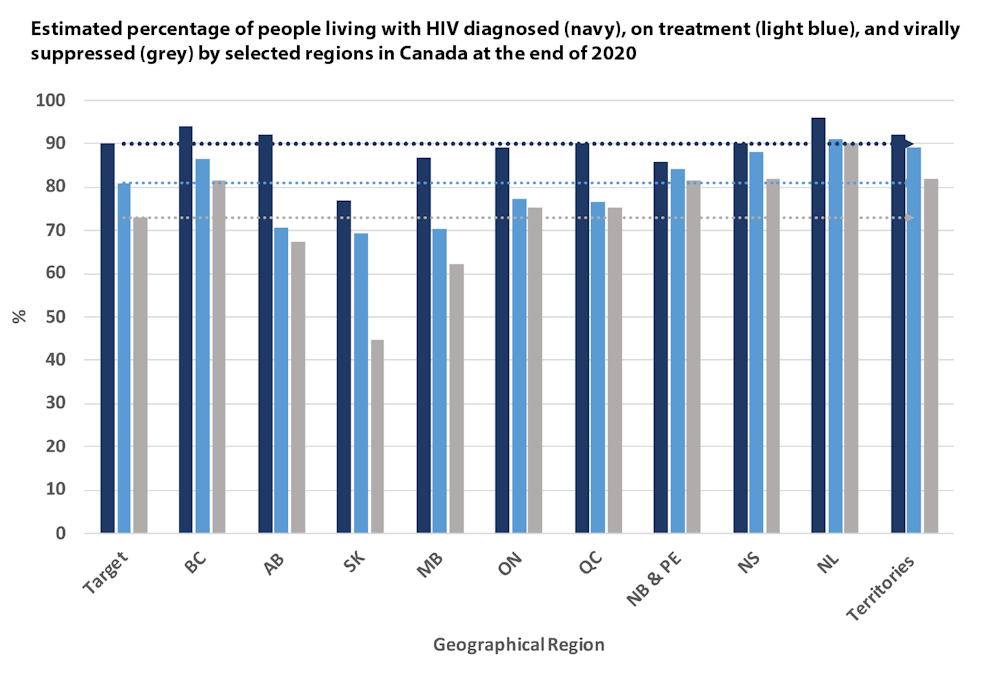
The reason for this discrepancy can be explained by the success of TasP in B.C., where the strategy originated. The graph below compares progress toward the UN’s 2020 target across Canada’s provinces and territories.
B.C., Nova Scotia, Newfoundland and Labrador and the three territories are the only Canadian jurisdictions that surpassed all three components of the benchmark target.
Estimated percentage of people living with HIV diagnosed, on treatment and virally suppressed by selected regions in Canada at the end of 2020.(Public Health Agency of Canada 2020 National HIV Estimates Report)
A failure to optimally implement TasP nationally has led to markedly different HIV rates across the country. In 2020, the national HIV incidence rate was 4.8 per 100,000 people. B.C., which had the highest domestic incidence rate at the peak of the epidemic in the 1980s, was well below the national average, at 2.5 per 100,000 population. The province is now at the low end of the national spectrum, together with the territories and Atlantic provinces at 2.1 and 2.2 per 100,000 population, respectively.
Alberta and Ontario were within the range of the national average at 4.2 and 4.1 per 100,000 population. At the other end, Saskatchewan, Manitoba and Québec were above the national average at 23.0, 7.7 and 5.8 per 100,000 population, respectively.
HIV rates in Canada by province and territory in 2020.(Public Health Agency of Canada 2020 National HIV Estimates Report)
What Canada needs to do
Clearly, Canada has the tools and the means to end the epidemic. The question remains, are we up to the task? The key requirements are well known:
Normalize HIV testing to ensure everybody knows their HIV status.
Expand support for affected populations, with particular emphasis on harder-to-reach and most affected populations (men who have sex with men, people dealing with substance use, sex workers, inmates, immigrants and First Nations Peoples).
Make free harm reduction services widely available (condoms, lubricants, injection and smoking paraphernalia, supervised injection and smoking consumption sites and safer drug supply programs).
Free relevant laboratory monitoring for all those on HAART or PrEP.
In addition, we must demand full transparency and accountability from our health-care system. That starts with PHAC annually reporting progress towards the UN 95-95-95 by 2025 target, HIV prevalence and AIDS-related mortality.
Finally, the federal government should sponsor a yearly independent summit of all relevant stakeholders to promote accountability and transparency, compare regional progress and share lessons learned in the process.
As a leader in treatment and prevention, Canada has a global responsibility to optimally implement a strategy to effectively combat HIV-AIDS. That will require a major commitment from the provinces given that health care is a provincial responsibility.
Canada knows how to end the HIV-AIDS epidemic. It is high time to get it done.
For workers in long-term care homes, distress due to difficult working conditions is often dismissed as a part of the job description. THE CANADIAN PRESS/Graham Hughes
Yet, wellness in the long-term care sector is rarely discussed. Distress due to difficult working conditions is often dismissed as a part of the job description. Workers are expected to “suck it up” and manage their own emotions on their own time.
The sector is currently being held together by a very vulnerable workforce and it is situated to fail without immediate intervention.
Support for self-care and protection from moral distress
In our research, we examined the impacts of two critical psychological safety factors on the long-term care workforce amidst the COVID-19 pandemic — support for self-care and protection from moral distress. Health-care workers expressed the increased need for resources to support their well-being and to address longstanding workforce issues. Five recommendations for a stronger long-term care sector are proposed.
1. Address long-standing structural issues
Structural issues have been brought to light during the COVID-19 pandemic. This includes issues that are economic, social and organizational in nature.
While the COVID-19 pandemic exacerbated the challenges facing the long-term care sector, workers stated that these issues are not new. Rather, decades of neglect and lack of funding has made low pay and unsafe working conditions acceptable.
A masked worker walks behind a hiring sign on his way into the Dover Cliffs long term care home in Port Dover, Ont. in November 2020.THE CANADIAN PRESS/Frank Gunn
The pandemic intensified existing problems with staffing shortages. In 2020, long-term care staff members made up more than 10 per cent of Canada’s total COVID-19 infection cases. Further, restricting informal caregivers from entering homes contributed to increased workloads.
Institutional support for any sort of resource (mental health, personal protective equipment (PPE), staffing) was stretched thin to keep care homes running. Resource limitations kept the hands of management teams tied, suggesting that distress was endemic across the sector.
2. Continuing education and training for self-care
Supporting staff through continuing education and training can increase their capacity for psychological self-care and help protect them from moral distress.
A resident holds hands with a health-care worker in a COVID-19 infected ward at Idola Saint-Jean long-term care home in Laval, Que. in February 2022.THE CANADIAN PRESS/Graham Hughes
Continuing education and training can significantly improve psychological well-being among long-term care workers. Communication-focused training approaches have resulted in improvements in staff turnover, depression and anxiety. Self-compassion and acceptance-based approaches found a significant reduction in mental health symptoms.
Educational sessions connect staff with other staff, allowing them to share their expertise and frustrations — helping to alleviate conflicts and tensions amongst teams. Virtual forums can be used for peer-to-peer learning, community building and moral support.
Training must be made available to all staff. Our study found that unregulated staff such as personal support workers were often not invited to take part in training programs or company resources.
3. Invest in leadership development
Improved leadership can foster improved team functioning.
Bullying and gossip is particularly rampant in the long-term care workplace. Workers expect one another to work through distress and asking for a day off can be seen as a weakness and increasing the workload for others.
Supportive managers are critical to the psychological well-being of staff. A study on transformative leadership found a reciprocal relationship between leadership, self-reported staff well-being, team efficacy and self-efficacy — leading to job satisfaction and well-being. Transformative leaders encourage employees to create change inwardly by connecting professional goals to a wider sense of belonging in their workplace.
Underfunding and resource constraints make it difficult to provide meaningful and accessible supports, reducing workers’ ability to protect themselves against moral distress in the workplace.
4. Ensure safe working conditions
Long-term care workers in PPE look out the window of a long term care home in Québec during the first wave of COVID-19 in 2020.THE CANADIAN PRESS/Graham Hughes
Insufficient personal protection equipment (PPE) at the workplace was a concern for workers in the sector. Staff shortages and lack of knowledge from management contribute to poor infection control and safety. Low wages and limited benefits also place workers in vulnerable situations, with limited options to practice physical and psychological self-care.
Funnelling resources and funding into this sector will not only improve staffing. It is critical for reducing the rapid turnover caused by uncontrolled exposure to COVID-19.
5. Supportive human resource policies
Long-term care needs to develop and/or improve human resource policies that support workers and acknowledge their value.
Low wages and precarious employment characterize this sector. Workers were fearful to take time off to get the COVID-19 vaccine for fear of losing wages.
Part-time and contract workers in the sector, often personal support workers, are not eligible for medical benefits and must pay out-of-pocket for injuries incurred at work. Many of these workers are racialized, immigrant women. Workers also often do not have entitlement to paid sick days. These factors point to systemic discrimination and undervaluing compared to other professionals in the sector.
A call to action
The Royal Society of Canada argues that the very first step to tackling the long-term care crisis is through workforce reform and redesign. This not only addresses low wages and resource shortages but serves more importantly to rebuild trust and dignity. To bolster support for the sector, public awareness and advocacy play a key role in advancing health-care reform.
Eight migrants from Somalia cross into Canada from the United States by walking down a train track into the town of Emerson, Man., in February 2017. THE CANADIAN PRESS/John Woods
Refugee advocates have long known about systemic problems with immigration enforcement in Canada, resulting in wrongful detentions and deportations, as well as people being tortured upon return to their countries of origin.
Flaws in Canada Border Services Agency’s (CBSA) structure and mandate mean that misconduct is tolerated and even incentivized. Independent oversight of CBSA and legislative changes are needed to protect refugee rights.
Deportation affects refugee rights
Our findings show that more than half the people deported from Canada each year made refugee claims. While some people are ready to return home, others still fear persecution.
People who are at risk of persecution, torture or worse can be denied refugee status and face imminent deportation. For these reasons, deportation is closely linked to refugee rights.
Asylum-seekers wait to be processed at the Canada Border Services Agency office in Lacolle, Que., in August 2017.THE CANADIAN PRESS/Ryan Remiorz
How someone is treated during the deportation process matters. CBSA places an emphasis on “timely removals” at the expense of respecting rights. And although Canada prides itself on its safeguards, they are insufficient.
But in 2012, the government introduced legislation that limits access to the pre-removal risk assessment. Since then, people can only apply for it if they remain in Canada for at least a year after their refugee claim was refused.
Our research found that whether someone is deported before the end of that year comes down to chance, defeating the very purpose of the risk assessment.
CBSA not equipped for sensitive work
Deportation is sensitive work. Yet the CBSA lacks the structure and management controls to carry out activities with human rights implications.
We obtained job descriptions for senior leaders in CBSA who oversee enforcement. They do not mention human rights treaties or obligations. There is no evidence that performance measures for leaders, front-line staff or the agency as a whole include compliance with international human rights obligations.
A Canada Border Services Agency patch is seen on an officer in Calgary, Alta.THE CANADIAN PRESS/Jeff McIntosh
Instead, CBSA documents emphasize the need for timely removals, specifically enforcing a deportation within one year of a refused refugee claim. Such fast deportations, as mentioned, may not leave refugee claimants with enough time to apply for the risk assessment.
Legal representatives we interviewed reported many instances of misconduct by CBSA officials, such as lying, abuse of power, concocting documents and baseless detentions to enforce a deportation. These tactics advance, rather than violate, CBSA’s mandate in the absence of requiring its employees to honour human rights obligations.
The CBSA also lacks an independent oversight body to review its work, investigate complaints and make binding recommendations. That means complaints about the conduct of CBSA officers must be made to CBSA.
A complaint can work against the person being deported. Many refugee lawyers told us they don’t bother reporting misconduct.
Lydia, a refugee lawyer, told us:
“I’ve complained about CBSA officers over the years with absolutely no effect. In fact, several officers who lied under oath were promoted after they had engaged in really disreputable conduct. Why waste your time?”
Legal help beyond reach
The deportation process is complex and unpredictable. Delaying or preventing a deportation requires expert legal advice. But it’s not easy to get legal representation for deportation cases, especially on a tight timeline.
Deportation cases require intense effort over a short period of time. Many experienced refugee lawyers rarely take a deportation case unless it’s a pre-existing client.
While refugees in Ontario may be eligible for legal aid, it doesn’t cover the real number of hours it takes to vigorously pursue the case. Sathya, a refugee lawyer, told us:
“It’s literally the worst work in this field …. It wipes every single thing off your desk. You have to put aside everything, cancel all your evening plans because you’re going to be pulling all-nighters. It is very, very difficult.”
What’s more, legal fees for deportation cases are often thousands of dollars, which is unaffordable for many refugee claimants.
Addressing injustice in deportations
An agency that conducts deportations must respect human rights obligations and the Canadian Charter of Rights and Freedoms. CBSA job descriptions should be revised to require compliance, which should be measured in performance evaluations.
To further address bias, CBSA needs to institute an anti-racism strategy, like the Anti-racism Strategy 2.0 being implemented within Immigration, Refugees, and Citizenship Canada.
The Canadian government should repeal the one-year bar on a refugee claimant seeking a pre-removal risk assessment to ensure that people at risk of persecution are not deported.
Finally, given the life-or-death implications of their work, the CBSA needs independent oversight. The Liberal government has proposed a bill to introduce such a watchdog. That bill must be passed to ensure respect for refugee rights.
Subscribe our Email News Letter to get Instant Update at anytime
About Oases News
OASES News is a News Agency with the central idea of diseminating credible, evidence-based, impeccable news and activities without stripping all technicalities involved in news reporting.